
An Evidence-Based Master Guide to Causes, Symptoms, Diagnosis, Non-Surgical Treatment, Rehabilitation & Prevention.
- Your Comprehensive Resource for Understanding Sciatica, Recovering Naturally, and Preventing Future Episodes
Welcome to The Complete Guide to Sciatica, a comprehensive evidence-based educational resource developed by Aryan Physiotherapy, Osteopathy & Manipulation Clinic. This guide has been created to help patients, caregivers, healthcare professionals, students, fitness enthusiasts, and anyone experiencing sciatic nerve pain understand every aspect of sciatica—from its causes and symptoms to diagnosis, conservative treatment, rehabilitation, home exercises, ergonomics, prevention, and long-term recovery.
Unlike many online articles that provide brief or incomplete information, this master guide brings together current scientific evidence, international clinical guidelines, and practical rehabilitation strategies into one easy-to-understand resource. It explains the anatomy of the sciatic nerve, why pain develops, how different spinal and muscular conditions contribute to symptoms, and how evidence-based physiotherapy, osteopathy, manual therapy, exercise therapy, ergonomic correction, and lifestyle modification can help many individuals recover without surgery.
This guide also explores diagnostic methods such as physical examination, MRI, CT scan, X-ray, EMG, and nerve conduction studies, helping readers understand when each investigation is appropriate. It compares conservative and surgical management using current research and discusses recovery timelines, prognosis, recurrence prevention, and frequently asked patient questions.
Throughout the guide, our goal is not simply to explain sciatica but to empower readers with accurate, research-backed information that supports informed healthcare decisions. Every chapter has been written with a strong emphasis on patient education, safety, and practical application.
Whether you are experiencing new symptoms, recovering from a lumbar disc injury, exploring non-surgical treatment options, or looking to prevent future episodes, this guide aims to become your trusted companion throughout your recovery journey.
About This Master Guide
Sciatica is one of the most common causes of lower back and leg pain worldwide, affecting millions of people every year. Despite its prevalence, misconceptions about the condition often lead to delayed diagnosis, unnecessary fear, prolonged disability, or inappropriate treatment choices. Many individuals believe that all sciatica requires surgery or prolonged bed rest, while others ignore early warning signs until the condition significantly affects their quality of life.
This master guide has been carefully designed to bridge that knowledge gap.
Drawing upon internationally accepted clinical guidelines, peer-reviewed scientific literature, and contemporary rehabilitation principles, it presents a balanced, evidence-based approach to understanding and managing sciatica. Complex medical concepts have been translated into clear, patient-friendly language while maintaining scientific accuracy. The information reflects current recommendations from organizations such as the World Health Organization (WHO), the American Physical Therapy Association (APTA), the National Institute for Health and Care Excellence (NICE), and research published in leading journals of spine care, rehabilitation, and musculoskeletal medicine.
Rather than focusing solely on symptom relief, the guide emphasizes identifying and addressing the underlying causes of sciatic nerve irritation. Readers will learn how factors such as lumbar disc herniation, spinal stenosis, piriformis syndrome, poor posture, occupational stress, reduced physical activity, obesity, and lifestyle habits contribute to the development and persistence of sciatica. Equally important, the guide provides practical strategies to reduce pain, restore function, improve movement, prevent recurrence, and maintain long-term spinal health.
Each chapter builds progressively—from anatomy and biomechanics to diagnosis, conservative treatment, exercise rehabilitation, ergonomics, prevention, and recovery—creating a complete educational journey that supports informed decision-making and active participation in rehabilitation.
Prepared by Aryan Physiotherapy, Osteopathy & Manipulation Clinic, this guide reflects our commitment to evidence-based practice, patient education, and personalized rehabilitation.
Purpose of This Guide
- The objectives of this master guide are to:
- Provide scientifically accurate and evidence-based information about sciatica.
- Help patients recognize early symptoms and understand potential causes.
- Explain diagnostic methods and their appropriate clinical use.
- Present current evidence supporting conservative management before considering surgery in appropriate cases.
- Demonstrate the role of physiotherapy, osteopathy, manual therapy, exercise therapy, and rehabilitation in recovery.
- Promote safe home management, ergonomic practices, and healthy lifestyle habits.
- Reduce fear, myths, and misinformation surrounding sciatica.
- Encourage informed discussions between patients and healthcare professionals.
- Support long-term recovery through education, self-management, and prevention.
Understanding Sciatica
What Is Sciatica? Causes, Anatomy, Symptoms, and Why Early Diagnosis Matters?

Lower back pain is one of the leading causes of disability worldwide, affecting people of every age, profession, and lifestyle. Among the many conditions responsible for lower back pain, sciatica is one of the most frequently misunderstood. Many people use the term “sciatica” to describe any pain that travels into the leg. Others believe that surgery is inevitable once sciatica develops. Some think prolonged bed rest is the best treatment, while others ignore symptoms until daily activities become severely restricted.
In reality, sciatica is not a disease itself but a symptom of irritation, inflammation, or compression of the sciatic nerve or one of the nerve roots that form it. Understanding the true nature of sciatica is the first and most important step toward effective treatment and long-term recovery.
Millions of people around the world experience sciatica every year. The condition affects students, office workers, healthcare professionals, drivers, manual laborers, athletes, older adults, and even pregnant women. Sciatica can interfere with walking, standing, sitting, sleeping, exercising, working, and enjoying everyday life. It often creates emotional stress, anxiety about movement, reduced work productivity, and financial burden due to medical expenses and lost workdays.
The encouraging news is that most cases of sciatica improve with evidence-based conservative management. Early assessment, accurate diagnosis, individualized physiotherapy, appropriate exercise, ergonomic modifications, and patient education play a crucial role in recovery. Surgery is reserved for selected situations and is not required for the majority of patients.
This guide has been developed to provide clear, research-based information that empowers patients and families to make informed healthcare decisions. Throughout this chapter, you will learn what sciatica is, how it develops, why symptoms occur, who is at risk, and why early recognition and proper management are essential.
What Is Sciatica?
Sciatica refers to pain that follows the course of the sciatic nerve, the largest and longest peripheral nerve in the human body. Rather than being a diagnosis itself, sciatica is a clinical syndrome caused by irritation or compression of one or more lumbar or sacral nerve roots, most commonly involving the L4, L5, S1, S2, or S3 spinal nerve roots.
The sciatic nerve begins in the lower spine, travels through the pelvis and buttock, runs down the back of the thigh, and divides into branches that extend to the leg and foot. Because of this long pathway, irritation anywhere along its course can produce symptoms in multiple regions of the lower limb.
Patients commonly describe sciatica as:
Sharp or shooting pain
Burning pain
Electric shock-like sensations
Tingling or “pins and needles”
Numbness
Muscle weakness
Pain that radiates from the lower back into the buttock, thigh, calf, or foot
The intensity of symptoms varies widely. Some individuals experience only mild discomfort, while others may find it difficult to walk, stand, sit, or sleep comfortably. Symptoms often worsen with prolonged sitting, coughing, sneezing, bending forward, or lifting heavy objects because these activities can temporarily increase pressure around the affected nerve root.
It is important to understand that leg pain caused by sciatica usually originates from the spine or surrounding structures, even though the most painful area may be in the buttock, thigh, or calf. Treating only the painful area without identifying the underlying cause may delay recovery or lead to recurrence.
Understanding the Sciatic Nerve
The sciatic nerve is the largest nerve in the human body, measuring approximately 2 centimetres in diameter in adults. It is formed by the anterior (ventral) rami of the L4, L5, S1, S2, and S3 spinal nerves, which unite within the pelvis to create a single large nerve trunk.
From the pelvis, the sciatic nerve exits through the greater sciatic foramen, usually passing beneath the piriformis muscle. It then travels deep within the buttock, descends along the posterior aspect of the thigh, and typically divides near the knee into two major branches:
Tibial nerve
Common fibular (peroneal) nerve
These branches continue to supply sensation and movement to the lower leg, ankle, and foot.
Functions of the Sciatic Nerve
The sciatic nerve has two primary functions:
1. Motor Function
It supplies muscles responsible for:
Knee flexion
Hip extension (indirectly through hamstrings)
Ankle movement
Foot movement
Toe movement
Normal walking, climbing stairs, running, jumping, and maintaining balance depend on healthy sciatic nerve function.
2. Sensory Function
The sciatic nerve provides sensation to much of the:
Back of the thigh
Leg
Calf
Heel
Sole of the foot
Outer aspect of the foot
Portions of the lower leg
Damage or irritation can therefore produce pain, numbness, altered sensation, or weakness in these regions.
Why Is It Called “Sciatica”?
The term sciatica refers to the symptoms caused by irritation of the sciatic nerve, not to a specific disease. It is similar to how “headache” describes a symptom rather than a diagnosis.
Several different conditions can produce sciatica, including:
Lumbar disc herniation
Lumbar disc bulge
Degenerative disc disease
Spinal stenosis
Foraminal stenosis
Piriformis syndrome
Spondylolisthesis
Traumatic injury
Tumours (rare)
Infection (rare)
Pregnancy-related nerve compression
Because the underlying causes differ, successful treatment depends on identifying the exact source of nerve irritation rather than treating every patient in the same way.
Sciatica Is a Symptom—Not a Disease
One of the most common misconceptions is that sciatica itself is a disease.
In reality:
A disc herniation is a disease.
Lumbar spinal stenosis is a disease.
Piriformis syndrome is a condition.
Sciatica is the collection of symptoms produced when these conditions irritate or compress the sciatic nerve.
This distinction is clinically important because treatment should target the underlying pathology rather than merely suppress pain.
For example:
A patient with sciatica caused by a lumbar disc herniation may benefit from extension-based exercises, activity modification, and nerve mobilization.
A patient whose symptoms arise from piriformis syndrome may respond better to stretching, soft tissue techniques, and hip muscle rehabilitation.
A patient with spinal stenosis often requires a different exercise strategy focused on flexion tolerance and walking capacity.
Although the symptoms may appear similar, the rehabilitation approach varies according to the diagnosis.
Key Clinical Insight
Pain does not always indicate the location of the problem. In sciatica, the source of irritation is frequently located in the lumbar spine, while the most intense symptoms are felt much farther down the leg. Understanding this concept helps explain why a thorough physical examination is essential before beginning treatment.
Anatomy of the Lumbar Spine
To understand sciatica, it is essential to understand the structure of the lower back. The lumbar spine consists of five vertebrae (L1–L5) positioned between the thoracic spine and the sacrum. These vertebrae bear the majority of the body’s weight and permit bending, lifting, twisting, walking, and other daily movements.
Between adjacent vertebrae lie intervertebral discs, which function as shock absorbers. Each disc is composed of:
-
Annulus Fibrosus: A strong outer ring of collagen fibers that provides structural stability.
-
Nucleus Pulposus: A gelatinous central core that distributes compressive forces and allows flexibility.
The lumbar vertebrae are connected by facet joints, ligaments, muscles, and fascia that together maintain spinal stability while allowing controlled movement.
Running through the vertebral canal is the spinal cord, which continues as the cauda equina below the level of L1–L2. Individual nerve roots exit the spine through openings called the intervertebral foramina. These nerve roots eventually unite to form the sciatic nerve.
Because the lumbar spine supports substantial loads and undergoes repetitive movement throughout life, it is particularly susceptible to degenerative changes, disc injury, and mechanical stress.
How Sciatica Develops
Sciatica occurs when one or more lumbar or sacral nerve roots become irritated, inflamed, or compressed. Although many patients assume the pain originates in the leg, the primary source is frequently located within the lumbar spine.
The most common mechanism involves a lumbar disc herniation. Degeneration or injury can weaken the annulus fibrosus, allowing the nucleus pulposus to protrude outward. This protrusion may compress an adjacent nerve root while also triggering an inflammatory response. Both mechanical pressure and chemical inflammation contribute to pain.
Other conditions—including spinal stenosis, foraminal narrowing, spondylolisthesis, piriformis syndrome, trauma, or space-occupying lesions—may produce similar symptoms by reducing the available space around the nerve or altering its normal mobility.
Pain may initially be confined to the lower back but often progresses into the buttock, thigh, calf, or foot following the course of the affected nerve. Symptoms may fluctuate depending on posture, movement, inflammation, and the body’s healing response.
Types of Sciatica
Although commonly discussed as a single condition, sciatica has several clinical patterns.
Acute Sciatica
Symptoms persist for less than six weeks. Acute episodes are frequently associated with disc injury or sudden mechanical overload and often respond well to conservative care.
Subacute Sciatica
Symptoms continue for six to twelve weeks. Rehabilitation becomes increasingly important during this phase to restore function and prevent chronicity.
Chronic Sciatica
Symptoms persist beyond twelve weeks. Chronic cases often involve ongoing biomechanical dysfunction, persistent inflammation, muscular deconditioning, central pain sensitization, or unresolved structural pathology.
True Sciatica
True sciatica results from irritation of one or more lumbar or sacral nerve roots supplying the sciatic nerve.
Pseudo-Sciatica
Pain mimics sciatica but originates from other structures such as the sacroiliac joint, hip joint, gluteal muscles, or piriformis muscle rather than the sciatic nerve itself. Differentiating between these conditions requires careful clinical assessment.
How Common Is Sciatica?
Sciatica is among the most common causes of lower-limb pain in adults.
Research indicates:
-
Approximately 5–10% of individuals with low back pain experience clinically significant sciatica.
-
Lifetime prevalence is estimated at 10–40%, depending on the population studied.
-
Peak incidence occurs between 30 and 60 years of age, although younger athletes and older adults are also affected.
-
Men and women are both affected, though occupational exposures may influence prevalence.
In India, increasing sedentary lifestyles, prolonged computer use, long-distance driving, obesity, and reduced physical activity contribute to a growing burden of lumbar spine disorders.
Risk Factors
Several factors increase the likelihood of developing sciatica:
Non-Modifiable Factors
-
Increasing age
-
Genetic predisposition
-
Congenital spinal abnormalities
-
Previous lumbar spine injury
Modifiable Factors
-
Prolonged sitting
-
Poor posture
-
Weak core musculature
-
Obesity
-
Smoking
-
Physical inactivity
-
Repetitive bending and lifting
-
Whole-body vibration (e.g., professional driving)
-
Poor workplace ergonomics
-
Inadequate flexibility
-
Occupational overuse
Addressing modifiable risk factors is an important component of both treatment and long-term prevention.
Why Early Diagnosis Matters
Many individuals delay seeking professional advice, assuming symptoms will resolve spontaneously. Although many episodes improve with time, persistent or progressive nerve compression may lead to muscle weakness, reduced mobility, and diminished quality of life.
Early assessment enables clinicians to:
-
Identify the underlying cause.
-
Exclude serious pathology.
-
Determine whether imaging is necessary.
-
Develop an individualized rehabilitation plan.
-
Reduce pain and disability.
-
Lower the likelihood of chronic symptoms.
Prompt intervention also helps patients avoid unnecessary investigations and inappropriate treatments.
Natural Course of Sciatica
The prognosis for sciatica is generally favorable.
Current evidence suggests that most patients improve with conservative management, particularly when education, activity modification, exercise therapy, and individualized rehabilitation are introduced early.
Recovery varies according to:
-
Cause of nerve irritation
-
Severity of neurological involvement
-
Duration of symptoms
-
Overall health
-
Adherence to rehabilitation
-
Occupational demands
Surgery is reserved for selected cases, such as progressive neurological deficit, cauda equina syndrome, or persistent disabling symptoms despite appropriate conservative management.
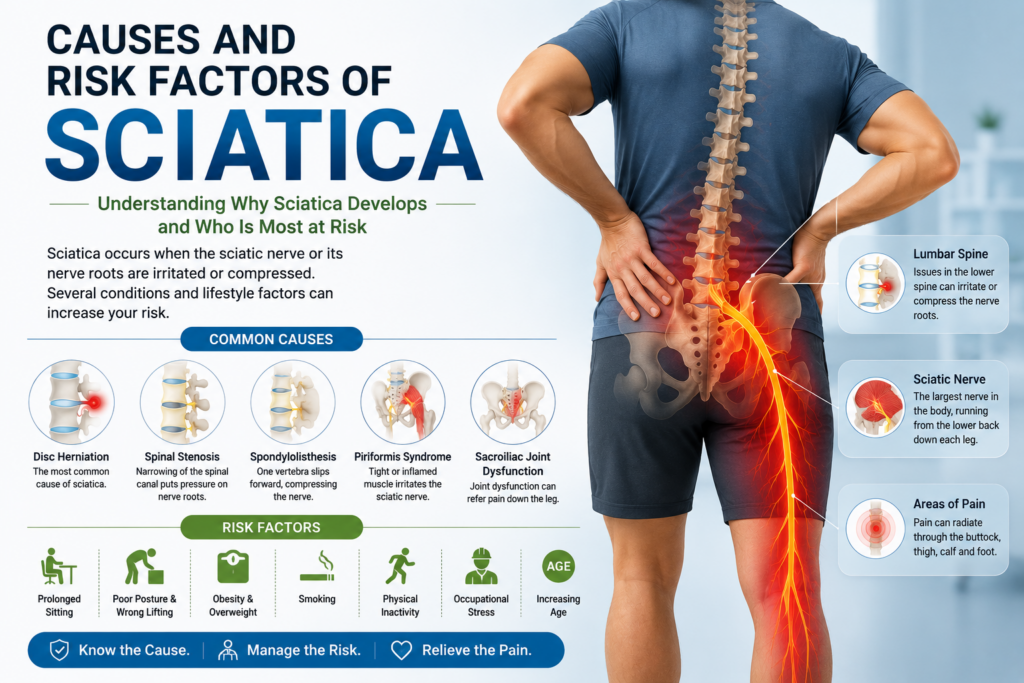
Causes and Risk Factors of Sciatica
Understanding Why Sciatica Develops and Who Is Most at Risk?
One of the most common questions patients ask is:
“What caused my sciatica?”
The answer is rarely simple.
Sciatica is not a single disease but rather a symptom that can arise from a variety of conditions affecting the lumbar spine, pelvis, or sciatic nerve. While a slipped disc is the most recognized cause, many individuals develop sciatica due to spinal degeneration, muscular dysfunction, poor ergonomics, prolonged sitting, occupational strain, or a combination of several contributing factors.
Understanding the underlying cause is one of the most important steps in treatment planning. Two patients may have nearly identical symptoms but require completely different rehabilitation strategies depending on the source of nerve irritation.
This chapter explains the major causes of sciatica, highlights important risk factors, and discusses how lifestyle choices can influence both recovery and recurrence.
What Causes Sciatica?
Sciatica develops when the sciatic nerve or one of its contributing nerve roots (L4–S3) becomes irritated, inflamed, compressed, or stretched.
The most common mechanisms include:
-
Mechanical compression
-
Chemical inflammation
-
Reduced nerve mobility
-
Degenerative changes
-
Muscular entrapment
-
Trauma
-
Space-occupying lesions (rare)
Pain may result from one mechanism alone or from a combination of factors.
1. Lumbar Disc Herniation
Lumbar disc herniation is the most common cause of sciatica, particularly in adults between 30 and 50 years of age.
An intervertebral disc consists of:
-
Annulus fibrosus (outer ring)
-
Nucleus pulposus (gel-like center)
With aging, repetitive loading, or injury, the annulus may weaken or tear. The nucleus can protrude outward, compressing a nearby nerve root.
Common Symptoms
-
Sudden lower back pain
-
Pain radiating below the knee
-
Tingling
-
Numbness
-
Weakness
-
Increased pain while coughing or sneezing
Most disc herniations improve without surgery when managed appropriately with education, activity modification, and rehabilitation.
2. Lumbar Disc Bulge
A disc bulge differs from a disc herniation.
In a bulge, the disc extends beyond its normal boundary without rupture of the outer fibers.
Many people have disc bulges on MRI without symptoms.
Sciatica occurs only when the bulge irritates or compresses the adjacent nerve root.
Clinical correlation is always more important than MRI findings alone.
3. Degenerative Disc Disease
As people age, spinal discs gradually lose water content and elasticity.
This natural aging process may lead to:
-
Reduced disc height
-
Less shock absorption
-
Increased mechanical stress
-
Foraminal narrowing
-
Nerve irritation
Not everyone with degeneration experiences pain.
Many age-related MRI changes are considered normal.
4. Lumbar Spinal Stenosis
Spinal stenosis refers to narrowing of the spinal canal.
Common causes include:
-
Arthritic changes
-
Thickened ligaments
-
Bone spurs
-
Disc degeneration
Patients often experience:
-
Leg pain while walking
-
Standing intolerance
-
Relief when sitting
-
Forward bending improves symptoms
This pattern is known as neurogenic claudication.
5. Foraminal Stenosis
Each spinal nerve exits through a small opening called the intervertebral foramen.
Degeneration can narrow this opening.
Compression of the exiting nerve root may produce:
-
Sciatica
-
Burning pain
-
Tingling
-
Weakness
Symptoms frequently worsen during spinal extension.
6. Spondylolisthesis
Spondylolisthesis occurs when one vertebra slips forward relative to another.
This may occur because of:
-
Degeneration
-
Stress fractures
-
Trauma
-
Congenital abnormalities
As the vertebra shifts, the exiting nerve root may become compressed.
Patients often report:
-
Back pain
-
Sciatica
-
Muscle tightness
-
Walking difficulty
7. Piriformis Syndrome
Not every case of sciatica begins in the spine.
The sciatic nerve passes close to the piriformis muscle.
Tightness, inflammation, or spasm of this muscle may compress the nerve.
Typical features include:
-
Buttock pain
-
Pain while sitting
-
Pain after prolonged driving
-
Tenderness over the buttock
-
Pain reproduced with hip rotation
This condition is sometimes referred to as deep gluteal syndrome.
8. Sacroiliac Joint Dysfunction
Pain originating from the sacroiliac joint may mimic sciatica.
Patients often experience:
-
Buttock pain
-
Groin pain
-
Posterior thigh pain
Unlike true sciatica, neurological symptoms are usually absent.
A detailed physical examination helps distinguish SI joint dysfunction from lumbar radiculopathy.
9. Facet Joint Syndrome
The lumbar facet joints guide spinal movement.
Arthritis or inflammation of these joints may refer pain into the buttock or thigh.
Although facet pain rarely extends below the knee, it may resemble sciatica during the early stages.
10. Pregnancy
Pregnancy places additional stress on the lumbar spine.
Factors include:
-
Increased body weight
-
Hormonal ligament laxity
-
Altered posture
-
Fluid retention
-
Pelvic changes
Many pregnant women experience symptoms resembling sciatica.
Fortunately, conservative management is usually effective.
11. Trauma
Falls
Road traffic accidents
Sports injuries
Heavy lifting accidents
Pelvic fractures
These injuries may damage discs, joints, ligaments, or directly affect the sciatic nerve.
12. Tumours and Infections
Although uncommon, serious conditions can produce sciatica.
Examples include:
-
Spinal tumours
-
Metastatic cancer
-
Epidural abscess
-
Vertebral infections
Red flags include:
-
Unexplained weight loss
-
Fever
-
Night pain
-
Progressive weakness
-
Bladder or bowel dysfunction
Immediate medical evaluation is essential.
Lifestyle Risk Factors
Several daily habits increase the likelihood of developing sciatica.
Prolonged Sitting
Office workers often remain seated for many hours.
This increases pressure within lumbar discs and reduces spinal movement.
Regular movement breaks every 30–45 minutes are recommended.
Poor Ergonomics
Incorrect workstation setup
Improper chair height
Laptop use without support
Poor driving posture
Improper lifting
These factors contribute to repeated spinal stress.
Obesity
Excess body weight increases mechanical loading on the lumbar spine.
Obesity is associated with higher rates of:
-
Disc degeneration
-
Low back pain
-
Sciatica
-
Osteoarthritis
Smoking
Smoking reduces blood supply to spinal discs.
It accelerates degeneration and delays tissue healing.
Smoking cessation benefits both spinal health and overall recovery.
Physical Inactivity
Weak core muscles
Poor endurance
Reduced flexibility
These factors decrease spinal stability and increase susceptibility to injury.
Occupational Risk Factors
Higher-risk occupations include:
-
Drivers
-
Office workers
-
Healthcare professionals
-
Factory workers
-
Construction workers
-
Warehouse employees
-
Farmers
-
Athletes
-
Gym trainers
Risk increases with repetitive lifting, prolonged vibration exposure, awkward postures, or sustained sitting.
Psychological Factors
Modern research recognizes that pain is influenced by more than structural changes alone.
Stress
Poor sleep
Anxiety
Depression
Fear of movement
Work dissatisfaction
These factors can increase pain sensitivity and delay recovery.
Addressing psychological well-being is an important component of comprehensive rehabilitation.
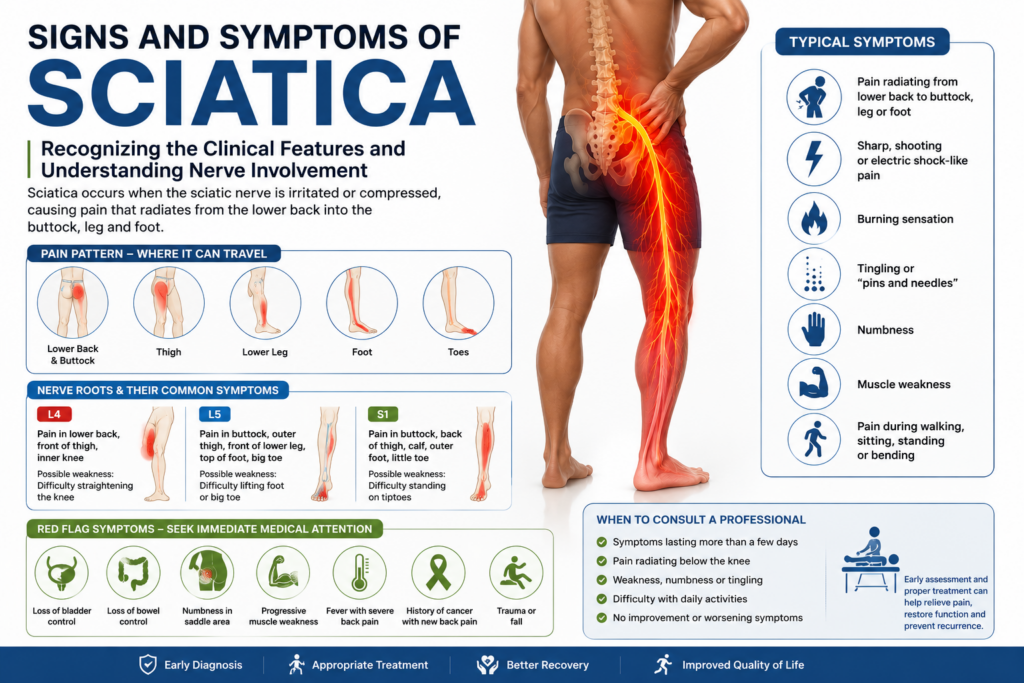
Signs and Symptoms of Sciatica
Recognizing the Clinical Features, Understanding Nerve Involvement, and Knowing When to Seek Medical Attention
One of the biggest misconceptions about sciatica is that every pain travelling into the leg is sciatica. In reality, several musculoskeletal, neurological, vascular, and hip-related conditions can produce symptoms that resemble sciatic nerve pain. Accurate recognition of the characteristic signs and symptoms is therefore essential for selecting the most appropriate treatment and avoiding unnecessary investigations or interventions.
Sciatica most commonly develops when one or more nerve roots contributing to the sciatic nerve become irritated or compressed. The resulting symptoms are not confined to the lower back. They frequently extend into the buttock, thigh, leg, or foot, following the anatomical course of the affected nerve.
The severity of symptoms varies considerably. Some individuals experience only occasional discomfort, while others struggle with walking, sleeping, working, or performing daily activities. Understanding the pattern of symptoms can help identify the likely level of nerve involvement and guide clinical decision-making.
Why Do Symptoms Vary?
The sciatic nerve originates from several spinal nerve roots (L4, L5, S1, S2, and S3). Each nerve root supplies a distinct area of skin (dermatome), muscles (myotome), and reflexes. Therefore, symptoms differ depending on which nerve root is affected and the degree of irritation.
For example:
-
Compression of the L5 nerve root often causes pain radiating to the outer leg and top of the foot, sometimes accompanied by difficulty lifting the big toe.
-
Compression of the S1 nerve root frequently produces pain down the back of the leg into the outer foot and may reduce the ankle reflex.
Typical Signs and Symptoms of Sciatica
Common symptoms include:
-
Pain radiating from the lower back to the buttock and leg
-
Sharp, shooting, or electric shock-like pain
-
Burning sensation
-
Tingling (“pins and needles”)
-
Numbness
-
Muscle weakness
-
Difficulty standing for prolonged periods
-
Pain during walking
-
Pain while sitting
-
Reduced spinal mobility
-
Night discomfort in some individuals
Symptoms usually affect one leg, although bilateral symptoms may occur in more serious conditions requiring urgent evaluation.
Characteristics of Sciatica Pain
Patients describe sciatica in different ways:
Sharp Pain
A sudden stabbing sensation, often triggered by bending, lifting, coughing, or sneezing.
Burning Pain
A persistent burning or hot sensation extending into the leg.
Electric Shock-like Pain
Sudden radiating pain travelling rapidly down the limb.
Deep Aching Pain
A constant dull ache involving the lower back, buttock, or thigh.
Intermittent Pain
Symptoms appear during certain activities and improve with rest or changes in position.
Constant Pain
Pain persists regardless of posture and may indicate more significant nerve irritation.
Pain Distribution by Nerve Root
L4 Nerve Root
Pain may occur in:
-
Lower back
-
Front of the thigh
-
Inner knee
-
Medial leg
Possible findings:
-
Difficulty straightening the knee
-
Reduced knee reflex
L5 Nerve Root
Pain typically radiates to:
-
Buttock
-
Outer thigh
-
Front of the lower leg
-
Top of the foot
-
Great toe
Possible weakness:
-
Difficulty lifting the foot
-
Difficulty lifting the great toe
-
Foot drop in severe cases
S1 Nerve Root
Pain commonly extends through:
-
Buttock
-
Back of the thigh
-
Calf
-
Outer border of the foot
-
Little toe
Possible weakness:
-
Difficulty standing on tiptoes
-
Reduced ankle reflex
Sensory Symptoms
The sciatic nerve supplies sensation to much of the lower limb. Irritation may produce:
Tingling
Often described as “pins and needles.”
Numbness
Reduced ability to feel touch, pressure, or temperature.
Altered Sensation
Patients sometimes report:
-
Crawling sensations
-
Cold feelings
-
Burning skin
-
Tightness
-
Hypersensitivity
These symptoms often follow a dermatomal pattern corresponding to the affected nerve root.
Motor Symptoms
Nerve compression can affect muscle function.
Patients may notice:
-
Leg weakness
-
Difficulty climbing stairs
-
Difficulty walking uphill
-
Trouble lifting the foot
-
Reduced push-off while walking
-
Frequent tripping
-
Foot drop (in severe cases)
Progressive muscle weakness requires prompt medical assessment.
Changes in Reflexes
During neurological examination, clinicians assess tendon reflexes.
Common findings include:
Reduced Knee Reflex
May indicate L3–L4 involvement.
Reduced Achilles Reflex
Often associated with S1 nerve root compression.
Although reflex changes support the diagnosis, they are interpreted alongside the patient’s history and physical examination.
Functional Limitations
Sciatica affects more than pain. It can significantly reduce daily function.
Patients frequently report difficulty with:
Sitting
Prolonged sitting increases disc pressure and may aggravate symptoms.
Standing
Some individuals experience worsening pain after standing for several minutes.
Walking
Walking tolerance varies depending on the underlying cause. Disc-related sciatica may improve with walking, whereas spinal stenosis often worsens.
Sleeping
Pain may disturb sleep, especially when changing positions or lying on the affected side.
Driving
Prolonged driving combines sustained sitting and vibration, both of which may aggravate symptoms.
Work
Office workers, healthcare professionals, drivers, and manual labourers often experience reduced productivity due to pain.
Symptoms That Can Mimic Sciatica
Not every radiating leg pain is true sciatica. Conditions that may present similarly include:
-
Piriformis syndrome
-
Sacroiliac joint dysfunction
-
Hip osteoarthritis
-
Greater trochanteric pain syndrome
-
Peripheral neuropathy
-
Vascular claudication
-
Hamstring injury
-
Facet joint syndrome
Accurate diagnosis requires a detailed history and physical examination.
Red Flag Symptoms
Certain symptoms require urgent medical attention because they may indicate serious neurological compromise.
Seek immediate medical evaluation if you experience:
-
Progressive muscle weakness
-
Loss of bladder control
-
Loss of bowel control
-
Saddle numbness (loss of sensation around the inner thighs or groin)
-
Severe pain following major trauma
-
Fever associated with severe back pain
-
Unexplained weight loss
-
History of cancer with new back pain
-
Night pain unrelated to movement
-
Rapidly worsening neurological symptoms
These findings may suggest conditions such as cauda equina syndrome, spinal infection, fracture, or tumour, all of which require urgent specialist assessment.
When Should You Consult a Physiotherapist?
Consult a physiotherapist if:
-
Leg pain persists for more than a few days.
-
Pain radiates below the knee.
-
Walking becomes difficult.
-
Daily activities are restricted.
-
Symptoms recur frequently.
-
Sitting or standing becomes uncomfortable.
-
You wish to avoid recurrent episodes through exercise and education.
Early physiotherapy assessment can identify movement impairments, postural factors, muscle weakness, and functional limitations, allowing a personalized rehabilitation program to be developed.
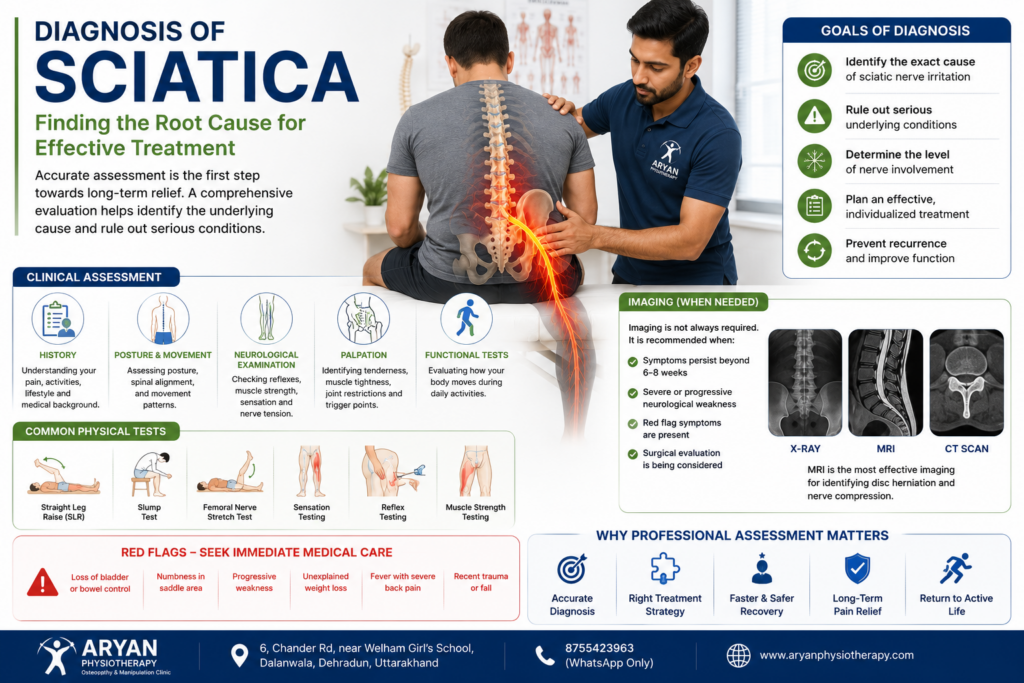
Diagnosis of Sciatica
Clinical Examination, Physical Tests, Imaging & Evidence-Based Diagnosis
One of the most common misconceptions among patients is that an MRI alone diagnoses sciatica. In reality, diagnosing sciatica requires a combination of a detailed medical history, physical examination, neurological assessment, and, when appropriate, imaging studies. Many individuals have disc bulges or degenerative changes visible on MRI without experiencing any symptoms. Conversely, some patients with significant sciatica may have only subtle imaging findings.
Accurate diagnosis helps determine the underlying cause of nerve irritation, identifies conditions requiring urgent intervention, and guides the selection of the most appropriate conservative or surgical treatment.
Why Accurate Diagnosis Matters
Sciatica can resemble several other musculoskeletal and neurological conditions. Misdiagnosis may lead to unnecessary investigations, delayed treatment, inappropriate exercises, prolonged pain, and avoidable healthcare costs.
An accurate diagnosis aims to:
Identify the exact source of nerve irritation.
Determine the severity of neurological involvement.
Exclude serious pathology.
Differentiate true sciatica from referred pain.
Develop an individualized rehabilitation plan.
Decide whether imaging or specialist referral is necessary.
Step 1: Patient History
A detailed history is often the most valuable diagnostic tool.
Your clinician may ask:
When did the pain begin?
Was there any injury or heavy lifting?
Does the pain travel below the knee?
Is one leg or both legs affected?
What activities make the pain worse?
What relieves the pain?
Do coughing or sneezing increase symptoms?
Is there numbness or tingling?
Have you noticed muscle weakness?
Have bladder or bowel habits changed?
Have you had previous episodes?
What treatments have you already tried?
The answers help identify whether the symptoms are mechanical, inflammatory, neurological, or potentially related to serious pathology.
Step 2: Pain Assessment
Pain assessment includes:
Location
Lower back
Buttock
Posterior thigh
Calf
Foot
Radiation
Pain extending below the knee is more suggestive of nerve root involvement.
Intensity
Pain may be assessed using:
Visual Analogue Scale (VAS)
Numeric Pain Rating Scale (NPRS)
Quality
Patients commonly describe pain as:
Sharp
Burning
Shooting
Electric shock-like
Aching
Throbbing
Duration
Acute (<6 weeks)
Subacute (6–12 weeks)
Chronic (>12 weeks)
Step 3: Red Flag Screening
Every patient should be screened for serious conditions.
Immediate medical evaluation is required if there is:
Progressive muscle weakness
Saddle anaesthesia
Loss of bladder control
Loss of bowel control
Fever
Unexplained weight loss
History of cancer
Severe night pain
Recent significant trauma
Suspected infection
These symptoms may indicate conditions such as Cauda Equina Syndrome, spinal tumour, vertebral fracture, or spinal infection.
Step 4: Physical Examination
A physical examination evaluates posture, movement, muscle strength, flexibility, and functional limitations.
Observation
The clinician assesses:
Standing posture
Lumbar curvature
Pelvic alignment
Walking pattern (gait)
Protective muscle spasm
Weight-bearing symmetry
Range of Motion
Lumbar movements assessed include:
Flexion
Extension
Side bending
Rotation
Restricted movement or pain reproduction provides valuable diagnostic information.
Step 5: Neurological Examination
A neurological examination evaluates nerve function.
Sensory Testing
Light touch and pinprick sensation are assessed along dermatomes to identify areas of altered sensation.
Motor Testing
Muscle strength is tested for:
Hip flexion
Knee extension
Ankle dorsiflexion
Great toe extension
Plantarflexion
Weakness may indicate involvement of specific nerve roots.
Reflex Testing
Common reflexes include:
Reflex Nerve Root Patellar Reflex L3–L4 Achilles Reflex S1 Reduced or absent reflexes may support the diagnosis of nerve root compression.
Step 6: Special Orthopaedic Tests
Straight Leg Raise (SLR)
The patient lies on their back while the examiner raises the affected leg.
Pain reproduced between 30° and 70° of hip flexion may indicate lumbar nerve root irritation.
The SLR is highly sensitive but not highly specific.
Crossed Straight Leg Raise
The unaffected leg is raised.
If pain occurs in the opposite symptomatic leg, the test has a high specificity for lumbar disc herniation.
Slump Test
Performed in sitting, this test places tension on the nervous system by combining spinal flexion, knee extension, and ankle dorsiflexion.
It is useful for detecting neural mechanosensitivity.
Femoral Nerve Stretch Test
Primarily evaluates upper lumbar nerve roots (L2–L4) and anterior thigh symptoms.
Step 7: Imaging Investigations
Imaging should be guided by clinical findings rather than routine use.
X-ray
Useful for assessing:
Fractures
Alignment
Degenerative changes
Spondylolisthesis
X-rays do not visualize nerves or intervertebral discs well.
MRI (Magnetic Resonance Imaging)
MRI is the investigation of choice when:
Symptoms persist despite appropriate conservative treatment.
Progressive neurological deficits develop.
Surgery is being considered.
Serious pathology is suspected.
MRI provides excellent visualization of:
Disc herniation
Nerve root compression
Spinal stenosis
Soft tissues
Ligaments
Infections
Tumours
However, MRI findings should always be interpreted alongside the patient’s symptoms and examination.
CT Scan
CT is useful when MRI is contraindicated or when detailed bony anatomy is required.
Step 8: Electrodiagnostic Studies
Electromyography (EMG)
Assesses muscle electrical activity to detect nerve injury.
Nerve Conduction Studies (NCS)
Evaluate the speed and quality of nerve signal transmission.
These tests are particularly helpful when:
Diagnosis is uncertain.
Peripheral neuropathy is suspected.
Symptoms persist despite treatment.
Differential Diagnosis
Several conditions may mimic sciatica:
Piriformis Syndrome
Sacroiliac Joint Dysfunction
Hip Osteoarthritis
Trochanteric Pain Syndrome
Peripheral Neuropathy
Vascular Claudication
Hamstring Injury
Lumbar Facet Syndrome
Meralgia Paresthetica
A careful examination helps distinguish these conditions.
Evidence-Based Conservative Management of Sciatica
Why Most Patients Recover Without Surgery?
For decades, many people believed that once sciatica developed, surgery was the only permanent solution. Fortunately, modern medical research tells a very different story.
Today, international clinical guidelines consistently recommend conservative (non-surgical) management as the first-line treatment for most patients with sciatica. Evidence from organizations such as the National Institute for Health and Care Excellence (NICE), the American Physical Therapy Association (APTA), the North American Spine Society (NASS), and systematic reviews published in The Lancet, BMJ, JOSPT, and Cochrane indicates that a large proportion of individuals recover successfully without surgery.
The emphasis of conservative management is not merely pain relief. Instead, it focuses on addressing the underlying mechanical, neurological, muscular, and lifestyle factors contributing to sciatic nerve irritation. Through education, movement, exercise, and individualized rehabilitation, patients are encouraged to regain function, restore confidence in movement, and reduce the risk of future episodes.
What Is Conservative Management?
Conservative management refers to non-surgical interventions aimed at reducing symptoms, restoring function, and improving quality of life. Rather than relying on a single treatment, it combines several evidence-based approaches tailored to the individual’s condition.
Conservative care may include:
Patient education
Activity modification
Physiotherapy
Osteopathy
Manual therapy
Therapeutic exercise
Neurodynamic (nerve-gliding) techniques
Ergonomic advice
Dry needling (where appropriate)
Weight management
Sleep optimization
Psychological support
Lifestyle modification
This comprehensive approach recognizes that sciatica is influenced by biological, mechanical, psychological, and social factors.
Is Conservative Treatment Effective?
Research consistently shows that most people with sciatica improve without surgery.
Studies indicate that many patients experience significant improvements in pain and function within 6–12 weeks, provided they receive appropriate assessment, education, and rehabilitation.
Recovery depends on several factors, including:
Cause of nerve irritation
Severity of symptoms
Duration of symptoms
Neurological involvement
Overall health
Physical activity
Adherence to rehabilitation
It is important to understand that recovery timelines vary. Some patients improve rapidly, while others require several months of structured rehabilitation.
Goals of Conservative Management
The objectives of treatment are to:
Reduce pain
Decrease inflammation
Improve nerve mobility
Restore normal movement
Improve spinal flexibility
Increase muscle strength
Improve posture
Enhance functional independence
Prevent recurrence
Improve quality of life
Reduce fear of movement
Promote long-term self-management
Pain relief alone should never be considered the only measure of success.
Patient Education: The Foundation of Recovery
One of the strongest predictors of successful rehabilitation is patient education.
Understanding the condition helps reduce anxiety, improves adherence to treatment, and encourages active participation in recovery.
Patients should understand:
What sciatica is
Why symptoms occur
Why movement is important
Why prolonged bed rest is not recommended
Why imaging is not always necessary
Expected recovery timelines
Warning signs requiring urgent review
Education transforms patients from passive recipients of care into active participants in rehabilitation.
Activity Modification
Many people ask:
“Should I rest until the pain disappears?”
Current evidence suggests that prolonged bed rest is generally not recommended for uncomplicated sciatica.
Instead, patients are encouraged to:
Continue normal activities as tolerated
Avoid activities that significantly increase symptoms
Walk regularly
Change positions frequently
Avoid prolonged sitting
Gradually return to work and exercise
Complete inactivity may contribute to muscle weakness, joint stiffness, reduced confidence, and delayed recovery.
Pain Management
Pain management should support movement rather than replace rehabilitation.
Depending on individual circumstances, strategies may include:
Heat therapy
Ice therapy
Gentle walking
Relaxation techniques
Breathing exercises
Sleep optimization
Physician-prescribed medication when appropriate
Pain should be monitored regularly using validated outcome measures to guide treatment progression.
Physiotherapy
Physiotherapy is a cornerstone of conservative sciatica management.
A physiotherapist performs a detailed assessment to identify:
Directional preference
Movement impairments
Muscle weakness
Joint stiffness
Neural mobility restrictions
Postural dysfunction
Functional limitations
Treatment may include:
Therapeutic exercise
Movement retraining
Manual therapy
Core stabilization
Balance training
Functional rehabilitation
Education
Ergonomic advice
Programs should be individualized rather than based on a one-size-fits-all approach.
Osteopathy
Osteopathy emphasizes the relationship between body structure and function.
An osteopathic assessment may examine:
Lumbar spine mobility
Pelvic alignment
Sacroiliac joint function
Hip mechanics
Fascial restrictions
Thoracic mobility
Treatment may include:
Joint mobilization
Soft tissue techniques
Muscle energy techniques
Myofascial release
Functional rehabilitation
Exercise prescription
Osteopathy is generally integrated with exercise and education rather than used as a standalone treatment.
Manual Therapy
Manual therapy refers to skilled hands-on techniques used to improve movement and reduce pain.
These may include:
Joint mobilization
Soft tissue mobilization
Myofascial release
Trigger point therapy
Spinal mobilization
Manual therapy is most effective when combined with active rehabilitation.
Patients should understand that hands-on treatment provides a window of opportunity for movement—it is not a substitute for exercise.
Neurodynamic Mobilization
Nerves must move freely during everyday activities.
Inflammation, scar tissue, or mechanical compression can reduce nerve mobility.
Neurodynamic techniques (nerve glides or nerve flossing) aim to:
Improve nerve mobility
Reduce sensitivity
Restore normal movement
Improve function
These exercises should be prescribed carefully to avoid symptom aggravation.
Exercise Therapy
Exercise is one of the most effective components of conservative care.
Depending on the diagnosis, exercises may focus on:
Lumbar mobility
Core strengthening
Hip strengthening
Gluteal activation
Hamstring flexibility
Nerve mobility
Balance
Functional movement
Exercise selection should always be individualized based on the patient’s presentation.
Dry Needling
Dry needling may be considered when muscle trigger points contribute to pain and movement restriction.
Potential benefits include:
Reduced muscle tension
Improved movement
Temporary pain reduction
Dry needling should always be performed by appropriately trained clinicians and integrated into a broader rehabilitation program.
Electrotherapy
The role of electrotherapy has evolved.
Modalities such as:
TENS
Interferential Therapy
Ultrasound
Laser therapy
may provide temporary symptom relief in selected patients. However, current evidence suggests they should not replace exercise, education, and active rehabilitation, which remain the primary drivers of long-term recovery.
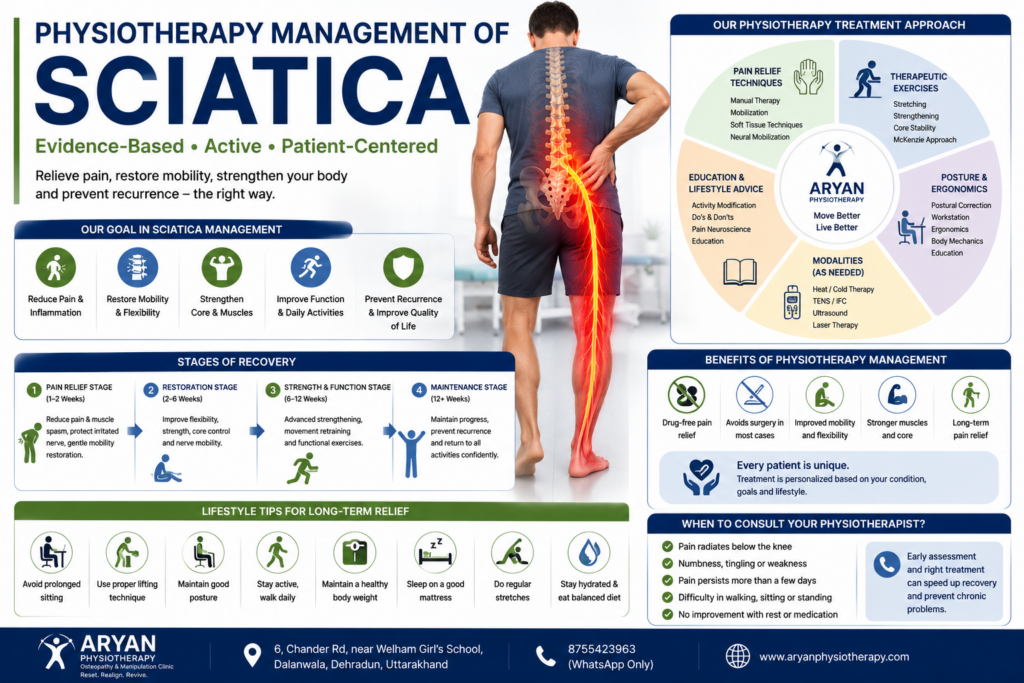
Ergonomic Correction
Daily habits influence spinal loading.
Patients should receive advice on:
Sitting posture
Standing posture
Lifting technique
Computer workstation setup
Driving position
Sleep positioning
Workplace ergonomics
Small ergonomic improvements can significantly reduce mechanical stress on the lumbar spine.
Lifestyle Modification
Recovery is influenced by overall health.
Important lifestyle factors include:
Maintaining a healthy body weight
Regular physical activity
Smoking cessation
Balanced nutrition
Adequate hydration
Stress management
Good sleep hygiene
These factors support tissue healing and reduce recurrence risk.
Psychological Factors
Pain is influenced by emotional and psychological health.
Fear of movement, anxiety, depression, poor sleep, and work-related stress can amplify pain and delay recovery.
A biopsychosocial approach recognizes that successful rehabilitation addresses both physical and psychological contributors to pain.
When Conservative Treatment Fails
Although most patients improve, further investigation or specialist referral may be appropriate when:
Progressive neurological weakness develops
Symptoms persist despite appropriate rehabilitation
Severe functional limitations remain
Red flag symptoms appear
Imaging identifies pathology requiring surgical opinion
Conservative treatment should always be reassessed and adjusted according to the patient’s progress.
Recovery Timeline
Recovery varies among individuals.
Typical progression may include:
Weeks 1–2
Pain control
Education
Activity modification
Gentle mobility
Weeks 3–6
Exercise progression
Core strengthening
Functional training
Weeks 6–12
Return to work
Sport-specific rehabilitation
Prevention strategies
Some individuals require longer rehabilitation depending on the underlying condition.
Physiotherapy Management of Sciatica
An Evidence-Based Rehabilitation Guide for Long-Term Recovery
Physiotherapy is one of the most researched and recommended treatments for sciatica. Current clinical guidelines from the American Physical Therapy Association (APTA), National Institute for Health and Care Excellence (NICE), North American Spine Society (NASS), and other international organizations recommend physiotherapy as a first-line conservative treatment for most individuals with sciatica.
The primary objective of physiotherapy is not simply to reduce pain, but to identify the mechanical, neurological, muscular, and functional factors contributing to symptoms. By addressing these underlying impairments, physiotherapy aims to restore movement, improve function, reduce recurrence, and help patients return confidently to their daily lives.
Effective physiotherapy is individualized. No single exercise or treatment works for everyone because sciatica has multiple causes. A thorough assessment guides the selection of interventions based on the patient’s diagnosis, symptoms, functional limitations, and personal goals.
Why Physiotherapy is the Gold Standard?
Modern physiotherapy follows a biopsychosocial model, recognizing that recovery depends on more than structural findings alone.
A physiotherapist evaluates:
Mechanical factors
Neurological involvement
Muscle performance
Joint mobility
Movement quality
Functional limitations
Occupational demands
Lifestyle habits
Patient beliefs and expectations
This comprehensive approach enables treatment to be tailored to the individual rather than the MRI report.
Goals of Physiotherapy
The goals of rehabilitation include:
Reduce pain
Improve nerve mobility
Restore lumbar mobility
Improve hip mobility
Increase core stability
Strengthen gluteal muscles
Improve flexibility
Restore walking tolerance
Improve sitting tolerance
Enhance work capacity
Restore sporting performance
Reduce recurrence risk
Improve confidence in movement
Promote long-term self-management
Initial Physiotherapy Assessment
Assessment forms the foundation of successful rehabilitation.
A comprehensive physiotherapy examination includes:
Subjective Assessment
The clinician gathers information about:
Pain onset
Mechanism of injury
Symptom behaviour
Aggravating factors
Easing factors
Previous episodes
Medical history
Occupational demands
Activity level
Patient goals
Observation
Assessment includes:
Standing posture
Sitting posture
Pelvic alignment
Lumbar curvature
Walking pattern
Functional movements
Movement Assessment
The following movements are examined:
Lumbar flexion
Lumbar extension
Side bending
Rotation
Hip mobility
Repeated movement testing may help identify a directional preference in selected patients.
Neurological Examination
The physiotherapist evaluates:
Dermatomes
Myotomes
Reflexes
Muscle strength
Sensation
Neural tension
Outcome Measures
To monitor progress objectively, validated outcome measures are recommended.
Examples include:
Numeric Pain Rating Scale (NPRS)
Visual Analogue Scale (VAS)
Oswestry Disability Index (ODI)
Roland-Morris Disability Questionnaire
Patient-Specific Functional Scale
Fear-Avoidance Beliefs Questionnaire
These measures help assess recovery over time and guide treatment adjustments.
Pain Management
Pain reduction is important, but it should facilitate movement rather than encourage inactivity.
Evidence-based strategies include:
Education
Activity modification
Heat therapy (where appropriate)
Ice therapy (in selected acute cases)
Gentle walking
Relaxation techniques
Breathing exercises
Passive treatments should complement—not replace—active rehabilitation.
Manual Therapy
Manual therapy may help reduce pain and improve movement in selected patients.
Common techniques include:
Lumbar mobilization
Thoracic mobilization
Hip mobilization
Soft tissue mobilization
Myofascial release
Trigger point therapy
Muscle energy techniques
Current evidence suggests manual therapy is most effective when combined with exercise and patient education.
Therapeutic Exercise
Exercise is the cornerstone of physiotherapy management.
The program should be individualized based on:
Diagnosis
Symptom severity
Directional preference
Functional goals
Physical capacity
Exercises may include:
Lumbar mobility exercises
Hip mobility exercises
Core strengthening
Gluteal strengthening
Balance training
Functional strengthening
Walking programs
Progression should occur gradually and according to symptom response.
Neurodynamic Mobilization
Healthy nerves glide and stretch during movement. In sciatica, this mobility may be reduced.
Neurodynamic techniques (nerve glides or nerve flossing) are designed to:
Improve nerve mobility
Reduce neural sensitivity
Restore normal movement
Improve function
Exercises should be performed within a comfortable range and progressed under professional guidance.
Core Stabilization
The core musculature—including the transversus abdominis, multifidus, diaphragm, and pelvic floor muscles—provides essential support for the lumbar spine.
Core rehabilitation focuses on:
Deep muscle activation
Motor control
Endurance
Functional integration
Examples include:
Abdominal bracing
Dead bug variations
Bird-dog exercises
Modified plank progressions
Improved core function enhances spinal stability and may reduce recurrent episodes.
Gluteal Rehabilitation
Weak or poorly coordinated gluteal muscles can increase stress on the lumbar spine and pelvis.
Strengthening exercises may include:
Bridges
Clamshells
Side-lying hip abduction
Squats
Step-ups
Hip thrusts
Functional single-leg exercises
Gluteal rehabilitation is particularly important in individuals with prolonged sitting, poor pelvic control, or altered gait.
Flexibility Training
Reduced flexibility may contribute to movement restrictions.
Stretching may target:
Hamstrings
Hip flexors
Piriformis
Calf muscles
Lumbar fascia
Stretching should be gentle and individualized. Aggressive stretching into pain is generally discouraged.
Gait Re-education
Pain often alters walking mechanics.
Physiotherapy may address:
Step length
Pelvic control
Trunk movement
Foot placement
Walking endurance
Correcting gait abnormalities helps reduce compensatory stress on the spine and lower limbs.
Functional Rehabilitation
Treatment should extend beyond isolated exercises.
Functional training may include:
Sit-to-stand practice
Stair climbing
Squatting
Lifting mechanics
Carrying tasks
Reaching activities
Work simulation
Sport-specific movements
The aim is to restore confidence and independence in everyday activities.
Electrotherapy
Modalities such as:
TENS
Interferential Therapy
Therapeutic Ultrasound
Low-Level Laser Therapy
may provide temporary symptom relief for selected patients. However, current evidence suggests that active rehabilitation remains the primary driver of long-term recovery.
Home Exercise Programme
A structured home programme reinforces clinic-based treatment.
Typical components include:
Walking
Lumbar mobility exercises
Core activation
Gluteal strengthening
Nerve glides
Hip mobility exercises
Stretching
Adherence is one of the strongest predictors of successful outcomes.
Return to Work
Returning to work should be gradual and individualized.
Recommendations may include:
Ergonomic adjustments
Frequent movement breaks
Modified duties
Progressive activity
Education regarding lifting techniques
Early return to appropriate work is often beneficial and should be encouraged when safe.
Return to Sports
Athletes require progressive rehabilitation emphasizing:
Strength
Power
Agility
Balance
Endurance
Sport-specific movement patterns
Return-to-sport decisions should be based on functional performance rather than pain alone.
Recovery Timeline
Recovery varies according to diagnosis and individual factors.
Typical progression:
Weeks 1–2
Pain management
Education
Gentle movement
Activity modification
Weeks 3–6
Progressive strengthening
Core rehabilitation
Functional exercises
Weeks 6–12
Advanced strengthening
Return to work
Sport-specific training
Prevention strategies
Some patients require longer rehabilitation depending on symptom duration and underlying pathology.

Osteopathy, Manual Therapy & Chiropractic Management of Sciatica
An Evidence-Based Comparison of Hands-On Therapies for Sciatic Nerve Pain

Sciatica is more than a compressed nerve—it often involves changes in spinal movement, muscle function, fascia, joint mechanics, posture, and nervous system sensitivity. For this reason, many treatment plans include hands-on therapies alongside exercise and patient education.
Three commonly discussed approaches are:
Physiotherapy
Osteopathy
Chiropractic
Although they share some techniques, they differ in philosophy, assessment, and clinical emphasis. Current research suggests that no single hands-on therapy is universally superior. The best outcomes are generally achieved when these approaches are integrated with exercise therapy, patient education, ergonomic advice, and active rehabilitation, rather than used in isolation.
The Evolution of Conservative Spine Care
Historically, spinal pain was often treated with prolonged bed rest, traction, or passive modalities. Modern rehabilitation has shifted toward evidence-based, active care, where manual techniques are used to reduce pain and improve movement, creating an opportunity for patients to participate in therapeutic exercise.
Today, international guidelines recommend:
Education
Exercise
Activity modification
Individualized rehabilitation
Manual therapy as an adjunct—not a standalone cure
Understanding Hands-On Therapy
Hands-on therapy includes techniques performed directly by a trained clinician to influence joints, muscles, fascia, ligaments, and the nervous system.
Potential goals include:
Reduce pain
Improve joint mobility
Decrease muscle tension
Improve tissue flexibility
Restore movement
Reduce fear of movement
Facilitate participation in exercise
These treatments are tools, not cures. Their value lies in supporting active rehabilitation.
What Is Osteopathy?
Osteopathy is a patient-centered healthcare approach that emphasizes the relationship between structure and function. It recognizes that restrictions in joints, muscles, fascia, and connective tissues may influence movement and contribute to pain.
In sciatica, osteopathic practitioners evaluate the body as a whole rather than focusing only on the painful area. The assessment may include:
Lumbar spine
Thoracic spine
Pelvis
Sacroiliac joints
Hips
Lower limbs
Rib cage
Fascial continuity
Breathing mechanics
The objective is to restore efficient movement and reduce unnecessary mechanical stress on the nervous system.
Principles of Osteopathy
Core principles include:
The body functions as an integrated unit.
Structure influences function.
The body has inherent healing potential.
Movement quality is essential for health.
Treatment should be individualized.
Modern osteopathy integrates these principles with current evidence-based rehabilitation.
Osteopathic Assessment
A comprehensive osteopathic assessment typically includes:
Patient History
Pain behaviour
Injury mechanism
Occupation
Activity level
Previous episodes
Observation
Posture
Pelvic alignment
Walking pattern
Movement quality
Palpation
Assessment of:
Muscle tone
Fascial tension
Joint mobility
Tissue sensitivity
Functional Movement
Evaluation of:
Lumbar movement
Hip mobility
Thoracic rotation
Pelvic mechanics
Functional tasks
The goal is to identify contributing movement impairments rather than focusing solely on imaging findings.
Osteopathic Treatment Techniques
Depending on clinical findings, treatment may include:
Joint Mobilization
Gentle oscillatory movements designed to improve mobility and reduce pain.
Muscle Energy Techniques (MET)
The patient actively contracts muscles against resistance to improve joint motion and reduce muscle tightness.
Myofascial Release
Techniques targeting fascial restrictions that may influence movement.
Soft Tissue Techniques
Massage-like methods addressing muscle tension and circulation.
Functional Techniques
Positioning tissues in a comfortable direction to reduce pain and improve mobility.
Craniosacral Approaches
Some osteopathic practitioners use craniosacral techniques; however, evidence for sciatica management remains limited and they should not replace evidence-based rehabilitation.
Scientific Evidence for Osteopathy
Research suggests that osteopathic treatment may reduce pain and improve function in selected patients with low back pain and related disorders when combined with exercise and education.
Current evidence indicates:
Moderate support for short-term pain relief.
Improvement in mobility.
Enhanced patient satisfaction.
Best outcomes when integrated with active rehabilitation.
Evidence does not support osteopathy as a standalone replacement for exercise.
What Is Manual Therapy?
Manual therapy refers to skilled hands-on techniques used by physiotherapists, osteopaths, chiropractors, and other trained clinicians.
Unlike a specific profession, manual therapy is a group of techniques.
Common goals include:
Improve movement
Reduce pain
Restore joint mechanics
Improve soft tissue mobility
Types of Manual Therapy
Joint Mobilization
Gentle repetitive movements applied within the joint’s normal range.
Joint Manipulation
A high-velocity, low-amplitude thrust applied to selected joints by appropriately trained clinicians.
Soft Tissue Mobilization
Techniques addressing muscles and fascia.
Myofascial Release
Manual treatment directed toward fascial restrictions.
Trigger Point Therapy
Pressure applied to painful muscular trigger points.
Neural Mobilization
Movement techniques designed to improve nerve mobility.
Scientific Evidence for Manual Therapy
Systematic reviews indicate that manual therapy can:
Reduce short-term pain
Improve spinal mobility
Enhance participation in exercise
Improve function
However, manual therapy alone is generally less effective than manual therapy combined with exercise and education.
This is why modern rehabilitation emphasizes a multimodal approach.
What Is Chiropractic?
Chiropractic is a healthcare profession primarily focused on the diagnosis and management of musculoskeletal disorders, particularly those involving the spine.
Chiropractic care commonly includes:
Spinal manipulation
Mobilization
Exercise advice
Lifestyle counselling
Ergonomic education
Although spinal manipulation is often associated with chiropractic, modern chiropractic practice may include a variety of conservative interventions.
Chiropractic Techniques
Common techniques include:
Diversified spinal manipulation
Flexion-distraction
Activator methods
Mobilization
Soft tissue techniques
Exercise prescription
Selection depends on patient presentation and clinician training.
Scientific Evidence for Chiropractic
Research suggests spinal manipulation may provide short-term improvements in pain and function for some patients with low back pain and sciatica.
Current evidence indicates:
Small to moderate improvements in selected patients.
Comparable outcomes to other conservative approaches in many studies.
Best results when combined with exercise and education.
Comparing Physiotherapy, Osteopathy & Chiropractic
Feature Physiotherapy Osteopathy Chiropractic Exercise Prescription Excellent Good Good Rehabilitation Excellent Good Moderate Manual Therapy Extensive Extensive Extensive Spinal Manipulation Selected cases Selected cases Common Functional Training Extensive Moderate Moderate Ergonomic Advice Extensive Good Good Patient Education Extensive Extensive Extensive Evidence for Sciatica Strong Moderate Moderate Integrated Rehabilitation
Rather than asking:
“Which profession is best?”
Modern rehabilitation asks:
“Which combination of evidence-based interventions best meets this patient’s needs?”
A comprehensive programme may include:
Education
Exercise
Physiotherapy
Osteopathy
Manual therapy
Ergonomic advice
Lifestyle modification
Psychological support when required
This integrated approach aligns with contemporary clinical guidelines.
Risks & Contraindications
Hands-on therapies are generally safe when performed by appropriately trained clinicians following a thorough assessment.
Treatment may not be appropriate in the presence of:
Fractures
Spinal infection
Malignancy
Severe osteoporosis
Cauda equina syndrome
Progressive neurological deficit
Certain inflammatory spinal conditions
A careful examination should always precede treatment.
Choosing the Right Treatment
Treatment should be based on:
Clinical findings
Patient goals
Severity of symptoms
Functional limitations
Medical history
Evidence-based practice
A collaborative, individualized approach generally provides the best outcomes.
Common Myths and Facts
Myth: Every case of sciatica requires surgery.
Fact: Most patients recover without surgery when managed appropriately.
Myth: Complete bed rest is the best treatment.
Fact: Prolonged bed rest may delay recovery. Controlled activity and appropriate exercise are generally recommended.
Myth: MRI is always required.
Fact: Imaging is not necessary for every patient and should be guided by clinical findings.
Myth: Leg pain means the problem is in the leg.
Fact: The underlying source is often located in the lumbar spine or pelvis.
Myth: Once sciatica develops, it will always return.
Fact: Many individuals recover fully and remain symptom-free with appropriate rehabilitation and lifestyle modification.
Myth: A slipped disc can simply be “put back into place.”
Fact: Disc tissue does not snap back into position through manipulation. Improvements are more likely related to reduced pain, improved movement, decreased muscle guarding, and natural healing.
Myth: You need spinal manipulation every week forever.
Fact: Long-term dependence on passive treatment is not supported by current evidence. The goal should be patient independence through education and exercise.
Myth: Hands-on therapy alone cures sciatica.
Fact: The strongest evidence supports combining manual techniques with exercise, education, and active rehabilitation.
Frequently Asked Questions
1. What is the main cause of sciatica?
Lumbar disc herniation is the most common cause, although spinal stenosis, piriformis syndrome, spondylolisthesis, and other conditions may also compress or irritate the sciatic nerve.
2. Is sciatica a permanent condition?
No. Many patients recover completely with appropriate conservative treatment.
3. Can sciatica heal naturally?
Many mild cases improve over time, but structured rehabilitation often accelerates recovery and reduces recurrence.
4. Is walking beneficial?
For many patients, gentle walking within a comfortable pain range promotes circulation and mobility. Individual recommendations vary depending on the cause.
5. Should I avoid exercise?
No. Appropriate, evidence-based exercise is a cornerstone of conservative management. Exercises should be selected according to the underlying diagnosis and supervised when necessary.
6. Does everyone need an MRI?
No. MRI is recommended only when clinical findings indicate the need or when symptoms persist despite appropriate conservative management.
7. Can poor posture cause sciatica?
Poor posture alone rarely causes sciatica but may contribute to mecha
1. What is the most common cause of sciatica?
Lumbar disc herniation is the leading cause, though spinal stenosis, piriformis syndrome, and degenerative changes can also contribute.
2. Can prolonged sitting cause sciatica?
Prolonged sitting can increase pressure on the lumbar spine and aggravate symptoms, especially when combined with poor posture or an existing spinal condition.
3. Is a disc bulge always painful?
No. Many people have disc bulges without symptoms. A bulge causes sciatica only if it irritates or compresses a nerve root.
4. Can pregnancy cause sciatica?
Yes. Hormonal changes, increased body weight, and altered biomechanics during pregnancy can contribute to sciatica-like symptoms.
5. Does everyone with sciatica need surgery?
No. Most people improve with evidence-based conservative management, including physiotherapy, exercise, and education.
6. Can stress make sciatica worse?
Stress does not directly compress a nerve, but it can increase muscle tension, reduce pain tolerance, and influence recovery.
7. Can sciatica be prevented?
While not all cases are preventable, maintaining spinal health through exercise, ergonomic habits, healthy weight, and early treatment of back pain can reduce the risk.
1. Can sciatica cause only leg pain without back pain?
Yes. Some individuals experience primarily leg pain because irritation of the nerve root may produce symptoms farther along the nerve’s course than at the spine itself.
2. Why does sciatica often affect only one leg?
Most cases involve compression of a single nerve root on one side of the spine. Bilateral symptoms are less common and may indicate a more serious condition.
3. Is numbness normal with sciatica?
Mild numbness or tingling can occur due to nerve irritation. Progressive or widespread numbness should be assessed promptly.
4. Can sciatica cause muscle weakness?
Yes. If nerve compression affects motor fibres, weakness may develop in the muscles supplied by the affected nerve root.
5. Does coughing or sneezing make sciatica worse?
Yes. These activities temporarily increase pressure within the spinal canal and may aggravate nerve root irritation.
6. How do I know if my leg pain is sciatica or a muscle strain?
Sciatica usually follows a nerve distribution and may include tingling, numbness, or weakness. Muscle strains are typically localized and related to muscle activity. A clinical examination is the best way to distinguish between them.
7. When should I seek emergency care for sciatica?
Seek immediate medical attention if you experience loss of bladder or bowel control, saddle numbness, rapidly progressive weakness, or severe symptoms following major trauma.
1. Is an MRI necessary to diagnose sciatica?
Not always. Many cases can be diagnosed through a detailed history and physical examination. MRI is reserved for specific situations.
2. What is the best clinical test for sciatica?
The Straight Leg Raise Test is one of the most commonly used screening tests, but it should always be interpreted alongside other findings.
3. Can an MRI show sciatica?
MRI can identify structural causes such as disc herniation or spinal stenosis but cannot diagnose symptoms on its own. Clinical correlation is essential.
4. Why do some people have abnormal MRIs without pain?
Age-related spinal changes are common and may not produce symptoms. Imaging findings do not always reflect the source of pain.
5. What are red flag symptoms?
Loss of bladder or bowel control, saddle numbness, progressive weakness, fever with back pain, unexplained weight loss, or severe trauma require urgent medical evaluation.
6. Is EMG painful?
Some discomfort may occur during EMG, but the procedure is generally well tolerated and provides useful information about nerve and muscle function.
7. Should everyone with sciatica see a surgeon?
No. Most patients improve with conservative care. Surgical referral is considered only for selected cases based on symptoms, examination findings, and imaging results.
1. Can physiotherapy cure sciatica?
Physiotherapy helps many people recover by addressing movement impairments, improving strength, restoring function, and reducing recurrence risk. Outcomes depend on the underlying cause.
2. Is bed rest recommended?
Current evidence does not support prolonged bed rest for uncomplicated sciatica. Gentle movement is usually encouraged.
3. Are exercises safe during sciatica?
Yes, when prescribed according to the individual’s diagnosis and tolerance.
4. Does manual therapy help?
Manual therapy can improve pain and movement, particularly when combined with exercise and education.
5. Can osteopathy help sciatica?
Osteopathy may improve mobility and function as part of a comprehensive rehabilitation program.
6. Is surgery always better?
No. For most patients without serious neurological deficits, conservative care is recommended before considering surgery.
7. How long does recovery take?
Many individuals improve within 6–12 weeks, although recovery varies depending on the underlying cause and adherence to rehabilitation.
1. Can physiotherapy completely cure sciatica?
Physiotherapy aims to address the underlying mechanical and functional contributors to sciatica. Many people recover fully, although outcomes depend on the underlying diagnosis and individual circumstances.
2. How many physiotherapy sessions are needed?
The number of sessions varies based on symptom severity, diagnosis, functional goals, and response to treatment.
3. Are exercises painful?
Exercises should challenge the body without significantly increasing symptoms. Temporary mild discomfort may occur, but severe or worsening pain should be reported.
4. Can physiotherapy help avoid surgery?
Many patients improve with physiotherapy and do not require surgery. Surgical decisions should be individualized and based on clinical findings.
5. Should I continue exercising after recovery?
Yes. Continuing an appropriate exercise programme helps maintain spinal health and reduce the likelihood of recurrence.
6. Is bed rest recommended during physiotherapy?
Prolonged bed rest is generally discouraged. Remaining active within a comfortable range is usually recommended.
7. Can I return to sports after sciatica?
Many individuals successfully return to sport following structured rehabilitation, provided strength, mobility, and functional performance have been restored.
1. Is osteopathy effective for sciatica?
Osteopathy may improve pain and movement in selected patients, particularly when combined with exercise and education.
2. Is spinal manipulation safe?
For appropriately selected patients and when performed by trained clinicians, spinal manipulation is generally considered safe. It is not suitable for everyone.
3. Which is better: physiotherapy, osteopathy, or chiropractic?
Current evidence does not identify one as universally superior. Treatment should be individualized and integrated with active rehabilitation.
4. Can manual therapy replace exercise?
No. Manual therapy is most effective when it supports participation in a structured exercise programme.
5. How many sessions are usually required?
The number varies depending on the underlying condition, symptom severity, and response to treatment.
6. Will my disc go back into place after manipulation?
There is no evidence that spinal manipulation physically “puts a disc back.” Improvements are more likely due to changes in pain, muscle function, and movement.
7. Should I continue exercises after my pain improves?
Yes. Ongoing exercise helps maintain spinal health, improve function, and reduce the risk of recurrence.